
Since last Thursday I have been pouring over video transcripts and selecting key portions to assemble into a 10 minute video about our class Redesigning The Neonatal ICU. Our goal for this short film is to communicate how combining interdisciplinary design students, patients and clinicians can lead to meaningful innovation in healthcare. We will be screening the film at Grand Rounds, Lucile Packard early next year. So, my apologies as this is my excuse for not getting to the final class blog post sooner. Last Thursday afternoon was our last class, which was held at CAPE. Students had approximately 4 weeks to complete their final project for the class. I will outline below the projects and people behind them:
 Stork Wings® (Patent Pending 2014) by Neil Ulrich (BS Eng) Saul Lopez (MS Eng) and Melissa Runsten (Law) tackled the sensitive problem of privacy for parents and baby in a cramped open bay style NICU. The ethnography they conducted led them to a wall mounted screen (can mount to a standard hospital headwall system). This screen utilizes recyclable, disposable printed paper that has the feel of a textile. This material was seen while we visited the Healthcare Design Conference in San Diego and toured Patient Centered Design’s NICU prototype. The same paper is being used for curtains in single room designs. (see below) By using this type of material, we no longer need to worry about fabric curtains holding onto germs, or the costs of laundering ceiling curtains.
Stork Wings® (Patent Pending 2014) by Neil Ulrich (BS Eng) Saul Lopez (MS Eng) and Melissa Runsten (Law) tackled the sensitive problem of privacy for parents and baby in a cramped open bay style NICU. The ethnography they conducted led them to a wall mounted screen (can mount to a standard hospital headwall system). This screen utilizes recyclable, disposable printed paper that has the feel of a textile. This material was seen while we visited the Healthcare Design Conference in San Diego and toured Patient Centered Design’s NICU prototype. The same paper is being used for curtains in single room designs. (see below) By using this type of material, we no longer need to worry about fabric curtains holding onto germs, or the costs of laundering ceiling curtains.
Watch the videos below to see how it works.
![FullSizeRender[2]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender2-e1418256758791.jpg)
![FullSizeRender[4]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender4-e1418256778926.jpg)
Video Links:
stork_wings (Converted) Emergency Release Video
* * * * * * * * * *
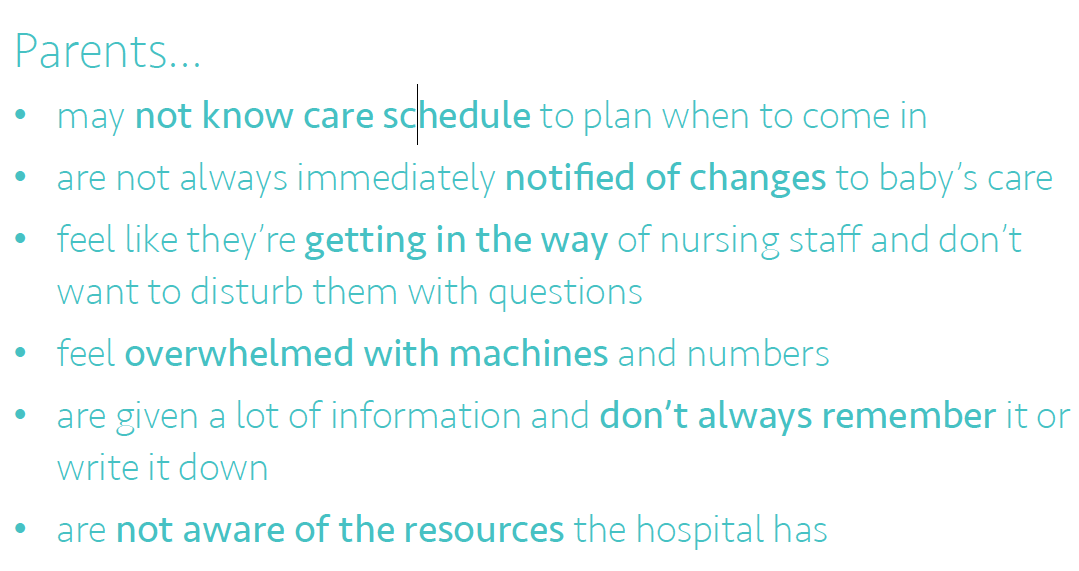
Parent Portal® by Evan Barry (MSE) , Olivia Wu (BS) and Jaikun Li (MS) were interested in helping parents feel more informed and comfortable by creating a place for them to organize their NICU experience. Here are the key problems this group uncovered through their user research:
![FullSizeRender[8]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender8-e1418320160447.jpg)
Their first prototype was made using paper and an app called POP.
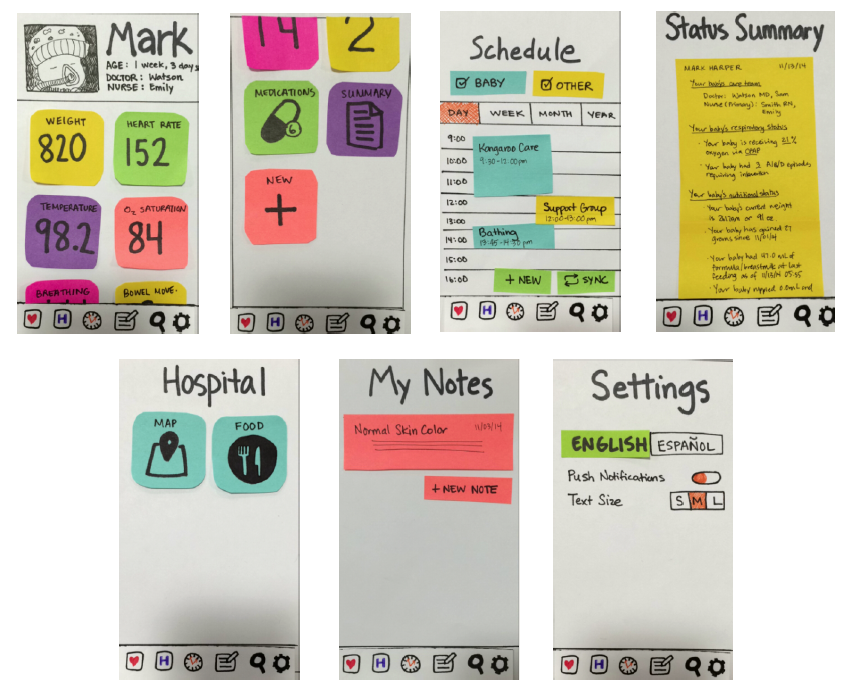
They received feedback from both clinicians and parents before they created a high resolution mobile solution.
* * * * * * * * * *
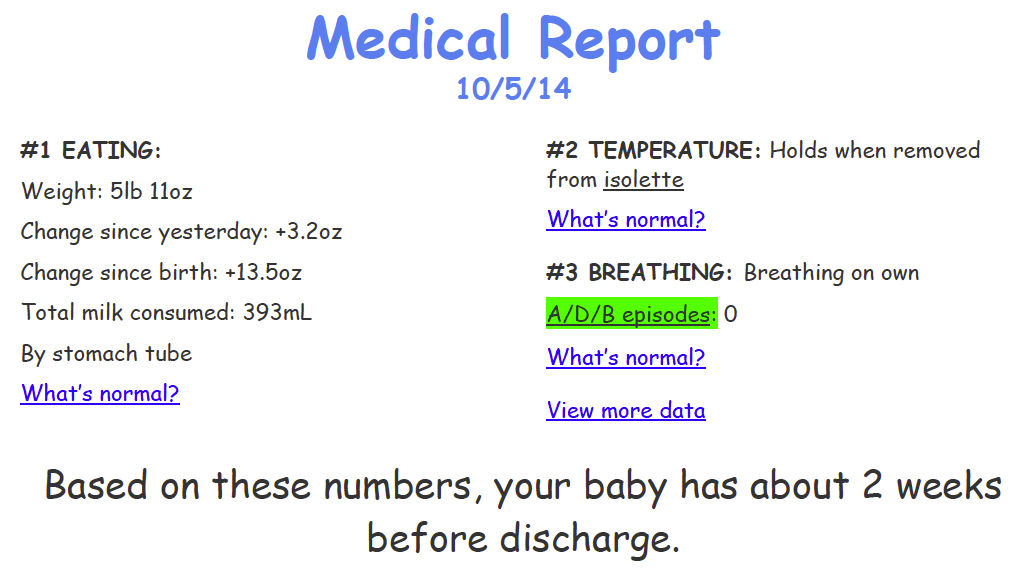
NICU Story by Rae Staben (BA Economics), Natalie Stottler (MS ME) and Justin Lee (MS CS) created a digital book or physical book with modifiable sections to assist parents in keeping track of their baby’s health conditions. This product focuses on condensing and displaying common medical jargon in the NICU in layman’s terms. Their goal was to create a better way to display daily reports (allowing for customizable information and progress reports), accommodate different outcomes and offer this product in a digital or paper format. Here is one image from their presentation:
Here are some images of NICU Story’s paper-prototype:
![FullSizeRender[1]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender11.jpg)
![FullSizeRender[2]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender21.jpg)
![FullSizeRender[3]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender31-e1418258809460.jpg)
* * * * * * * * * * * * *
NICU to Home Transitional Care by Maryam Attai (PhD Education), Suhui Chen (MS) and Stephen Jacobson (MS) tackled the issues around parents conquering anxiety and developing care competency with their baby before being discharged.
Through their interviews and direct observation in the NICU, they learned that parents need a way to prepare for their child’s transition from the NICU to home. They found that parents worried about taking their baby away from constant medical supervision and needed to feel more confident as parents and primary caregivers. Their work centered around creating the opportunity to practice caring for one’s baby as one would at home while still in the NICU. They expored the following HMW statements:
¤How might we provide the educational information parents want and feel they need to effectively care for their baby?
¤How might we offer more hands on care with the nursing staff until parents feel confident they know how to care for their baby when they go home?
¤How might we simulate common transition scenarios so parents can practice resolving them with guidance from the baby’s medical team?
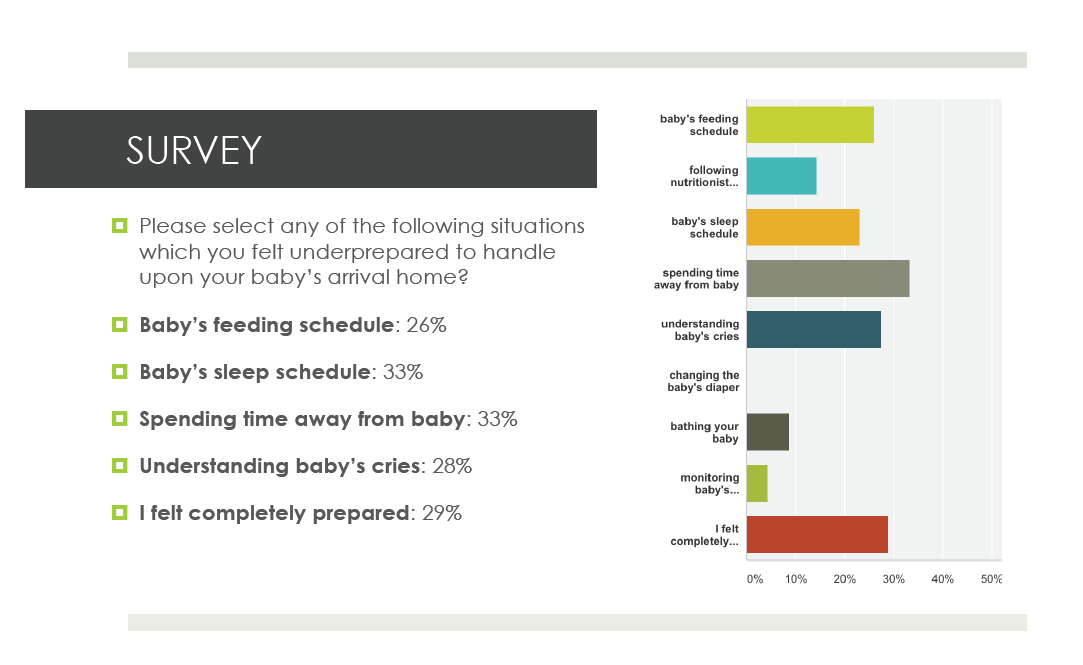
They created a survey with 81 NICU parents through foundation organizations in order to understand what the top parent concerns were before discharge. Here is what they found:
1.) Spending time away from baby (anxiety about leaving the baby with another caretaker)
2.) Understanding baby’s cries
3.) Baby’s feeding schedule
4.) Baby’s sleep schedule
To me this project seemed like it could become part of a “Standard of Care.” Similar to Dr. Robert White’s “NICU Standard’s” document. For example, implementation of protocols used in this training program could be part of obtaining Baby Friendly Hospital designation. By spending time training parents to better handle the challenges ahead at home, post-discharge, hospitals also lower their readmissions numbers saving money in the long run. This team took it a step further by performing a skit in CAPE’s clinical space to better show how transitional care might be carried out at the hospital.
![FullSizeRender[4]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender41.jpg)

* * * * * * * * * *
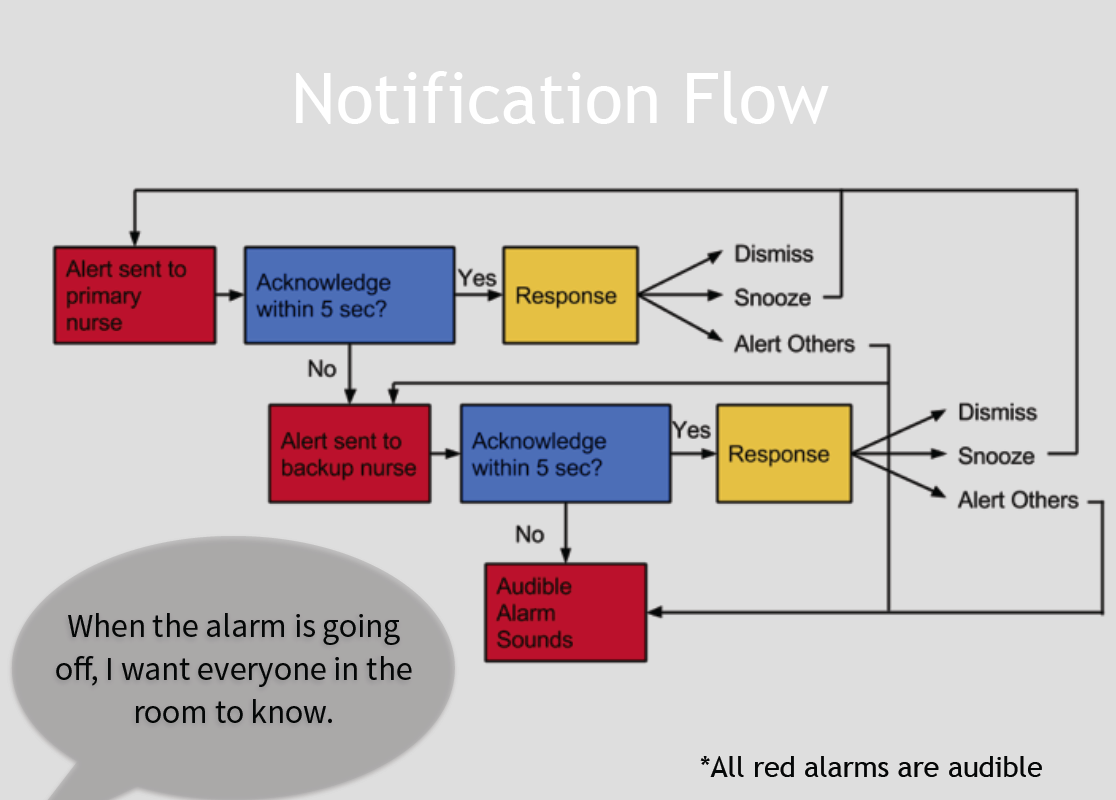
The NICU Noise Project by Cesare Jenkins (PhD EE), Josh Feler (MS) and Hyun Seung Hong, addressed the problems of the various alarms that are constantly going off in the NICU, 40% of which are false alarms. Their point of view was that nurses need a better way to receive alerts about the babies in their care because audible alarms are information poor, cause anxiety for parents and contribute to a loud NICU environment. To drive this point home further, The Joint Commission released its 2014 National Patient Safety Goal on Alarm Management in June 2013. By July 1, 2014, leaders need to establish alarm system safety as a hospital priority and identify the most important alarms to manage. In addition, by January 1, 2016, hospitals will be expected to develop and implement policies and procedures for managing alarms and to educate staff about the purpose and proper operation of alarms systems for which they are responsible. This group’s prototypes for managing alarms better ranged from a conceptual Google Glass® software application, to a wrist worn device (anything worn on the wrist is actually not allowed in the NICU as they quickly found out!), and finally a projected image that could instantaneously provide data regarding the alarms sounding and why, on the hand/arm of the clinician.



The projection would come from a small device that could be clipped to one’s pocket as they illustrate on the design in the lower right corner below. Currently, the tech isn’t small enough to fit into this designed enclosure, but within the next 2-3 years they feel it will be possible.

In addition to designing a new way to monitor and respond to these alarms, they also designed a new notification flow idea which was highly regarded by several clinicians in the room at our final critique:
* * * * * * * * * *
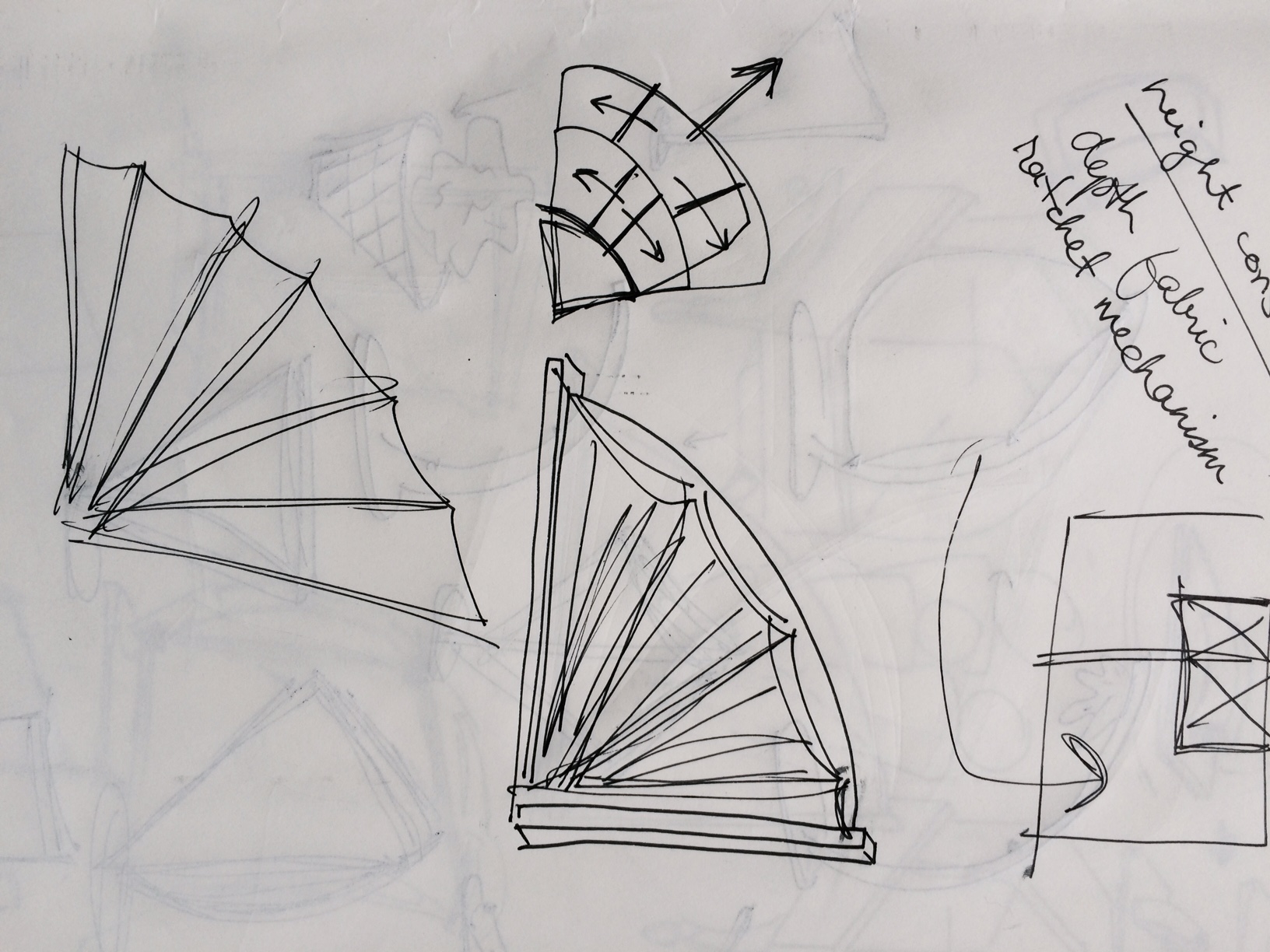
Kacoon® (Patent Pending 2014) by Abhishek Venkataramana (BS Biology) Graeme Fielder (MBA) and Mikkel Soerenson (Human-Computer Interaction) is a knock-down chair designed specifically for doing kangaroo care.
Click on the Kacoon link above for a short video describing their process and where they are today with the project. This group intends to push this project forward and I am so glad they are. As we all learned while visiting NICUs this past quarter, the hospital chairs that are currently being used for parents are either folding chairs with minimal padding or very large heavy “hospital grade” recliners that are expensive, difficult to move and take up a lot of space. This group was interested in creating a “knock-down” design that could be stowed when not in use and easily reassembled when a parent goes to the NICU to do Kangaroo Care with their baby. Below are a few of their exploratory sketches/prototypes:
![FullSizeRender[5]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender51-e1418320127254.jpg)
![FullSizeRender[6]](http://www.redesignhealthcare.org/wp-content/uploads/2014/12/FullSizeRender61-e1418320113605.jpg)


* * * * * * * * * *
Thanks for getting this far! I am very proud of our students and what they have learned this quarter in our class. The other night while reading student interview transcripts (about their class experience) I was thrilled to learn that for some students, this class was more than an immersive design and clinical experience, it was an opportunity to explore their own creativity, push aside perfection and jump into a field in which they had no knowledge, yet found they could develop meaningful solutions by “trusting the process”. What this means is learning to listen with the intent to understand, pulling out meaningful insights from this study, and using that information to create successful solutions.
A few quotes from our students:
What did you learn in this class that surprised you the most?
GRAEME: Probably something more about myself, coming from a very technical background and then going into sort of some other core fundamentals of business now in the business school, being able to exercise my own creativity and figure out that I can be creative is probably one of the biggest takeaways I’ve had, I think, and being able to show results of that creativity today.
MARYAM: I think this class is really amazing because it actually provides hands on experience. I know that there are a lot of classes that really strive to get students to feel like they’re immersed in an experience, but this course is different in that we were going to very unique environments. You know, it’s not every day that you take a course where you’re actually immersing yourself in a hospital critical care unit for neonatal babies. It’s not every day that you’re traveling to Kaiser Permanente Innovation Center to view their new semi-private NICU room prototype.
OLIVIA: I think this class gave me a lot of confidence in in pursuing bigger projects in the future, and how to approach a question that doesn’t have a straightforward answer.
* * * * * * * * * *
What’s next for me?
Last year I helped write the design portion of an NIH grant proposal with a group of clinicians at CAPE (Center for Advanced Pediatric & Perinatal Education). A few weeks ago we learned that the NIH has funded our projects! The proposal is called “Optimizing safety of mother and neonate in a mixed methods learning laboratory.” Our study is a collaboration of a multi-disciplinary team including investigators at Stanford and the University of California San Francisco. The primary work setting will be at CAPE’s simulation lab. I am in the “core” group and will be working P/T running focus groups, research, and developing prototypes once we have uncovered problems actionable through design. Dr. Louis Halamek and Dr. Henry Chong Lee are the primary investigators. There are four main projects that we will be working on:
Project #1: An optimal interactive display for neonatal resuscitation.
Project #2: An Optimal Data Display for Labor and Delivery
Project #3: Improving Recognition of Maternal Clinical Deterioration
Project #4: Physical design of the optimal delivery suite
I am also continuing to develop a lactation support product “Primo-Lacto: A Closed System For Colostrum Collection, with my amazing team Ryan Van Wert, MD and Rush Bartlett PhD, MBA
* * * * * * * * * *
Thanks to all for making this class a reality:
Stanford’s d. School, Dr. William Rhine, our fabulous students, CAPE Staff, Dr. Robert White, Mardelle Shepley, Dennis Boyle, Tammy Thompson, Dr. Louis Halamek, Dr. Parvati Dev, Dr. William Heinrichs, Brad Slaker, Dr. Nicole Yamada, Dr. Janene Fuerch-Hogan, Heather Keller, NICU Parents, LPCH NICU Staff, John Muir NICU Staff, The Kaiser Permanente Garfield Innovation Center, Design Coaches/Mentors, and Jan Sturmann (videographer). We could not have done this without you.